
Heart Block - An Electrical Travel Delay
In our last article we spoke about the malfunction of the Sinoatrial node (SA Node). The sinoatrial node is the physiological pacemaker of the heart and its dysfunction can lead to what is known as sick sinus syndrome. If you haven’t read that yet, here you go.
Now we are going to talk about another group of arrhythmias which are more commonly seen than sick sinus syndrome. These arrythimias are collectively known as heart blocks. The basic idea behind heart block is that the impulse that is generated by the sinus node does not reach the ventricles. This is because there is a block in the conduction pathway between the SA node and the ventricle. Grossly the blocks maybe classified into being complete or incomplete and being nodal or infra-nodal.
Before we continue our discussion of heart block, revise the basic ECG findings in a heart with sinus rhythm in this article.
Now to better understand heart blocks, lets think about an analogy.
Imagine a train going from City A to City B and it is carrying energy for City B. Without that energy City B cannot function properly. For a long time, this train is functioning completely normally and arrives at City B very regularly. (City A is the SA node and City B is the ventricles)
One day, the train conductor slows down a little in between for a brake and he shows up at city B a little late. Its not a big deal. Life goes on. (First Degree AV block - prolonged PR intervals)
In the following few days, the conductor takes longer and longer breaks on the way to City B. Finally, one day he doesn’t show up at all. (Second degree AV block - Mobitz type I - progressively prolonged PR intervals follwed by a dropped beat)
Now the people in City B are mad. They reprimand this conductor and tell him that if this happens again, he would lose his job. The conductor is scared and he goes back to work dilligently.
One fine day the conductor becomes frustrated with his job. And breaking his streak of regular deliveries and completely without warning, he decides to just not show up to City B! (Second degree AV block - Mobitz type II - normal PR intervals with a dropped beat)
Now the people in City B are furious. They say lets stop being dependent on City A and this useless conductor for our energy and make our own. So from that day onwards, City B functions autonomously irrespective of the arrival of the energy from City A. (Third Degree AV block or complete AV block- complete AV dissociation)

Now this is a very childish analogy but it really drives home the point of different types of heart block.
From an ECG perspective, there are three things that you need to identify to diagnose the type of heart block:
P wave
QRS complex
PR interval
First Degree AV block
There is a slowing of the conduction in the AV node and so PR interval is more than 200 msec
But the PR interval is the same from one beat to the next.
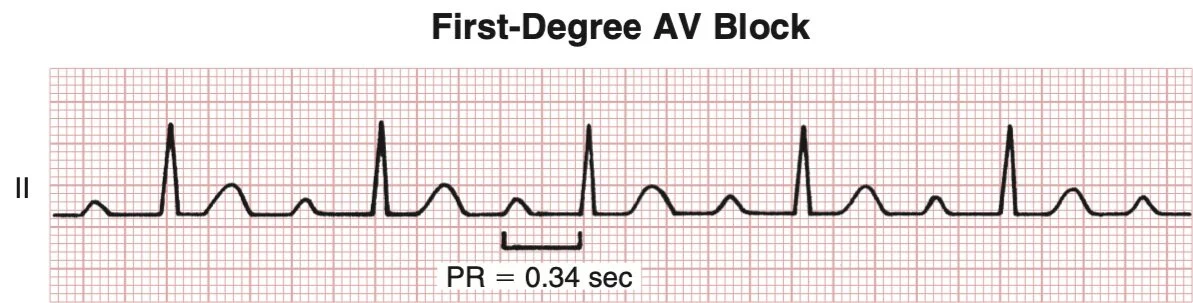
Note that the PR interval is prolonged (>o.2 sec) and that it is equal with each successive beat.
Reproduced from Goldberger’s Clinical Electrocardiography, 9th Edition.
Second degree AV block: Mobitz type 1
Also known as Wenkeback Phenomenon
There is progressive slowing of the conduction, which means, on the ECG, there is progressive lengthening of the PR interval
Eventually, the conduction is so slow that it does not conduct which results in a dropped beat on the ECG.

Note how there is progressive increase in the PR intervals in the first three beats. In the fourth beat, there is a P, but no QRS complex, signifying the dropped beat.
Reproduced from Goldberger’s Clinical Electrocardiography, 9th Edition.
Second Degree AV block: Mobitz type 2
In this type there is an intermittent failure to conduct an impulse.
There is no change in the PR interval
There is a regular sinus rhythm followed by a sudden missed beat.

Note how all the PR intervals are of the same duration. Two beats are followed by a missed beat without any evidence.
Reproduced from Goldberger’s Clinical Electrocardiography, 9th Edition.
Third Degree AV block
Also known as complete heart block.
In this case, there is no electrical communication between the SA node and the ventricles. The Artria conduct independently from the ventricles.
On the ECG there is complete dissociation of the P waves and the QRS complexes.

These are the individual findings of the heart blocks. Here is a good approach to them when you get an ECG and need to identify the kind of heart block.
The last thing to do, one a heart block has been identified is to identify the point of the block. The block may be either nodal, in which case the anatomic culprit is the AV node, or the block may be infranodal, in which case the anatomic culprit is somewhere below the AV node. Now identification of nodal or infranodal block is done by examining the morphology of the QRS complex. If the QRS complex is narrow (<0.12s) then its a nodal block. If the QRS complex is wide (>0.15s) then it is an infranodal pathology.
So now we know how to identify a heart block if we see one on an ECG. But what causes them? Most commonly heart blocks are caused by drugs or a myocardial infarction. But there are a few other causes as well, as shown in the table below.
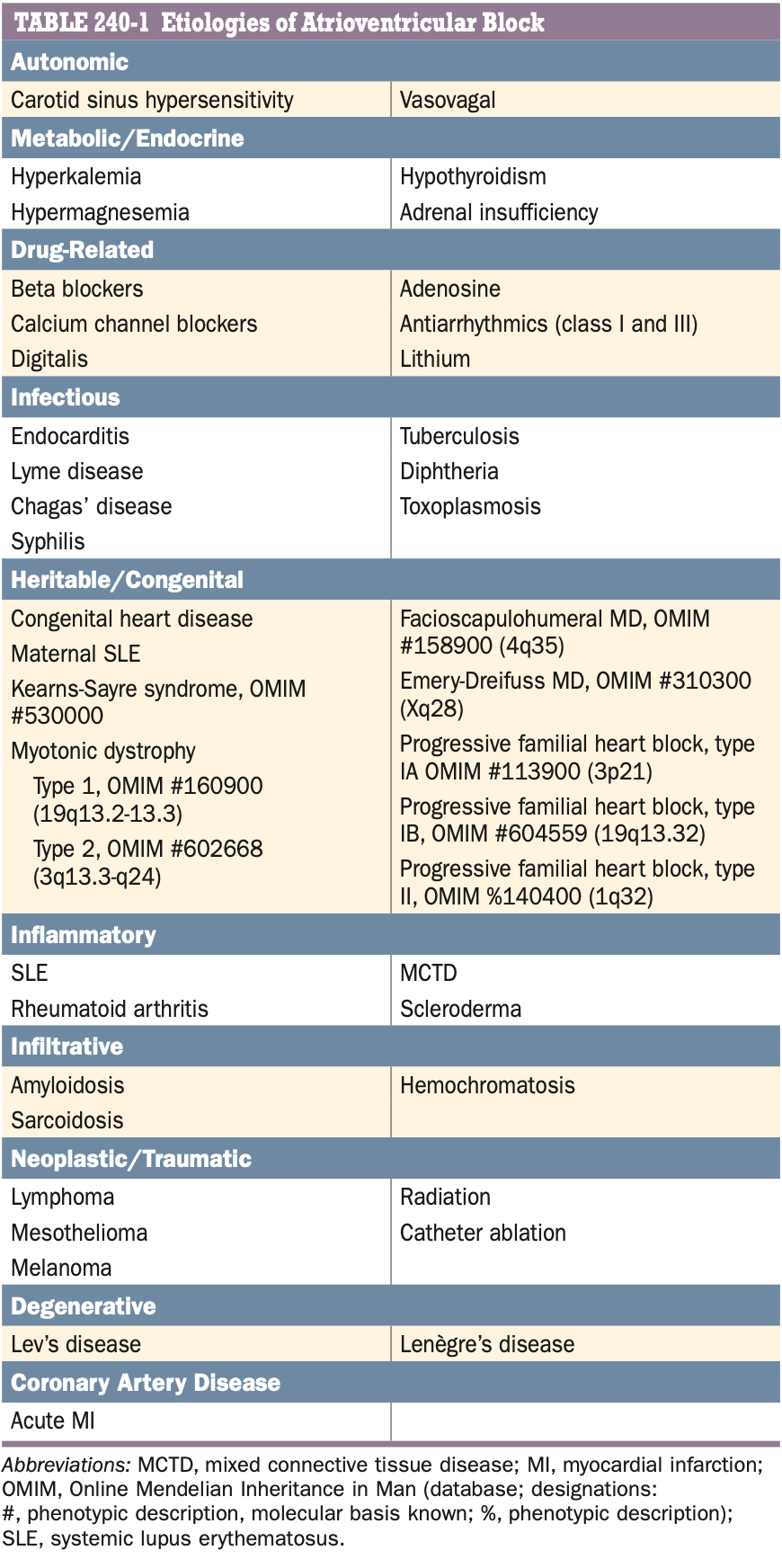
Causes of heart block or AV block
Reproduced from Harrison’s Principles of Internal Medicine, 20th edition.
Now, once we have identified a heart block, how do we treat it?
Most first degree heart blocks are left untreated unless they are symptomatic.
However, second or third degree heart blocks usually require pacing.
Initial medical treatment may be done with atropine or isoproterenol following which temporary pacing is done. Temporary pacing may be transcutaneous or transvenous. Finally permanent pacing is done.
Author: Narendran Sairam (Facebook)
Sources and citations